Both childhood obesity and eating disorders are at an all time high in our country today. According to the National Association of Anorexia Nervosa & Associated Disorders (ANAD), eating disorders are the third most common chronic condition in adolescents, after obesity and asthma.
Eating disorders are also the second deadliest mental illness, behind opioid addiction. The onset is typically during adolescence, with the highest prevalence in adolescent girls, but sadly eating disorders are increasingly being recognized in children as young as five to twelve years old.
On the other hand, childhood obesity has nearly doubled since the COVID pandemic. According to the U.S. Centers for Disease Control and Prevention, the prevalence of childhood obesity in the U.S. is about 20%.
In addition, the psychosocial morbidities associated with childhood obesity, such as depression, poor self-esteem, and poor quality of life, are of significant concern. There is much evidence that supports that if obesity prevention and treatment are not conducted correctly, the efforts could actually lead to development of eating disorders.
Initial attempts to lose weight by eating in a healthy manner may progress to severe dietary restriction, skipping of meals, prolonged periods of starvation, or the use of self-induced vomiting, diet pills, or laxatives.
2023 Clinical Guidelines on Childhood Obesity
In an attempt to decrease the childhood obesity rates, the American Academy of Pediatrics (AAP), updated its guidelines for evaluating and treating childhood obesity. They have moved away from “watchful waiting,” or delaying treatment to see if the children will outgrow obesity, to a more aggressive approach.
The AAP reports that the lifestyle changes are still the primary treatment, but if the preventative and healthy eating/exercise angle does not seem effective, the guidelines suggest even more drastic interventions.
They are now proposing that nutrition support, behavioral therapy, and exercise guidance aimed at weight loss should be starting as early as two years old. These interventions also include offering weight loss medications to kids 12 or older and considering bariatric surgery for teens 13 and older with severe obesity.
We are not talking about weight or size when speaking about childhood obesity.
The AAP uses body mass index (BMI) percentages to determine weight loss interventions. For children specifically, it is measured as a percentile between the child’s age and sex. A child higher than the 95th percentile is considered “obese”.
Unfortunately, the BMI itself does not take into account many important factors including muscle mass, bone density, or genetics.
It is my belief that these updated guidelines set up a perfect storm for eating disorders to flourish in our children. When we take children in larger bodies and a medical professional tells them that there is something wrong with their body, it can only set our children on a lifetime path of difficulty around food, weight, and disordered eating.
Weight Stigma In a Doctor’s Office Starts Young
Not only have rates of eating disorders and childhood obesity increased, but childhood weight stigma is rampant. When our children experience this stigma and shame, they may suffer from increased rates of depression, anxiety, poor body image and social isolation.
The rigidity, restriction, and over emphasis on weight can backfire and contribute to disordered eating behaviors and a poor relationship with food as the child grows up. Our children are still growing and developing in their childhood and adolescence, and during puberty this is an ultimate period of confusion for them.
We do not know which kids and adolescents are most vulnerable to the development of an eating disorder. Providers and families must remember that eating disorders are serious mental illnesses with significant morbidity, and it simply may start with negative comments about one’s body or weight.
The Impact of Others
I have had my own personal experience with an eating disorder in my past. I still remember my 9th grade annual physical for the swim team. After battling with binging and purging starting at 13 years old, I began the weight gain/loss cycle and gained 15 pounds in 6 months after initially losing weight from restricting my food intake.
My mom privately spoke to my pediatrician about her concern about my restricting/binge eating cycles and over exercise behaviors. I overheard the pediatrician tell my mom “She is actually slightly overweight for her height and weight, so those behaviors are really not a concern to me. I don’t see a concern for anorexia or bulimia at all.”
I still remember my feelings of shame, disgust, and rage. I told myself that I would lose weight and show her. That experience with a doctor I trusted was just one of the many catalysts that continued to fuel my eating disorder and self hatred as a teenager and young adult.
I grew up in a weight and appearance focused household mainly modeled by my mother, who focused on her weight, food intake, and appearance. I do not blame my mom, as she was raised the same way, probably even more strictly focused on her appearance determining her ultimate worth as a human being.
By the age of 7 years old, I was clear that what I weighed and looked like were extremely important and should be managed well in order to be accepted by my family and society. I struggled with an eating disorder from the age of 13 to 32 years old. I devoted my adolescence and young adult years to desperately trying to maintain the perfect weight and look perfect on the outside, meanwhile, I was dead on the inside.
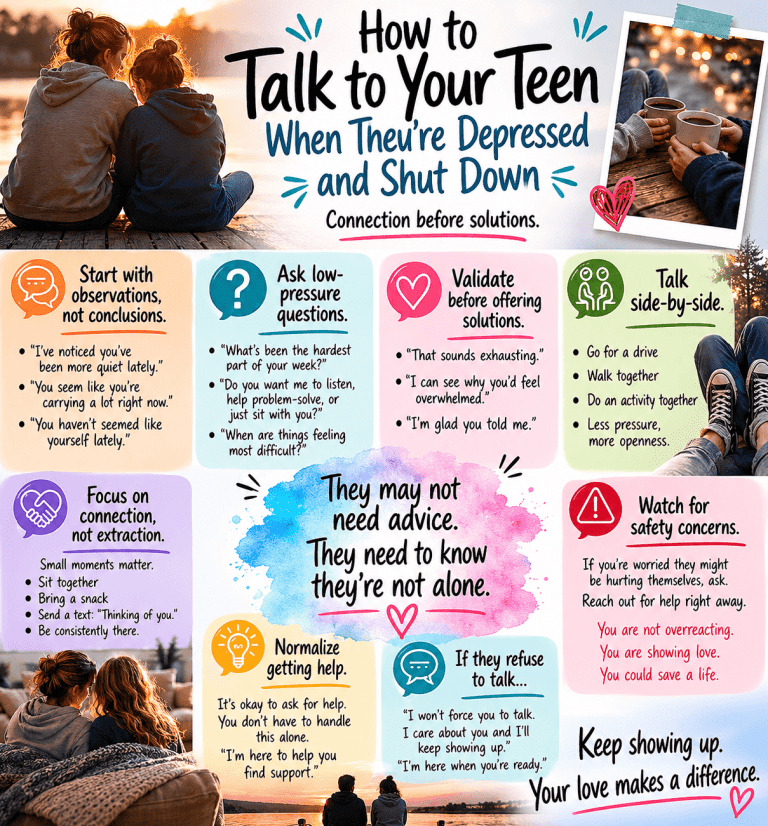
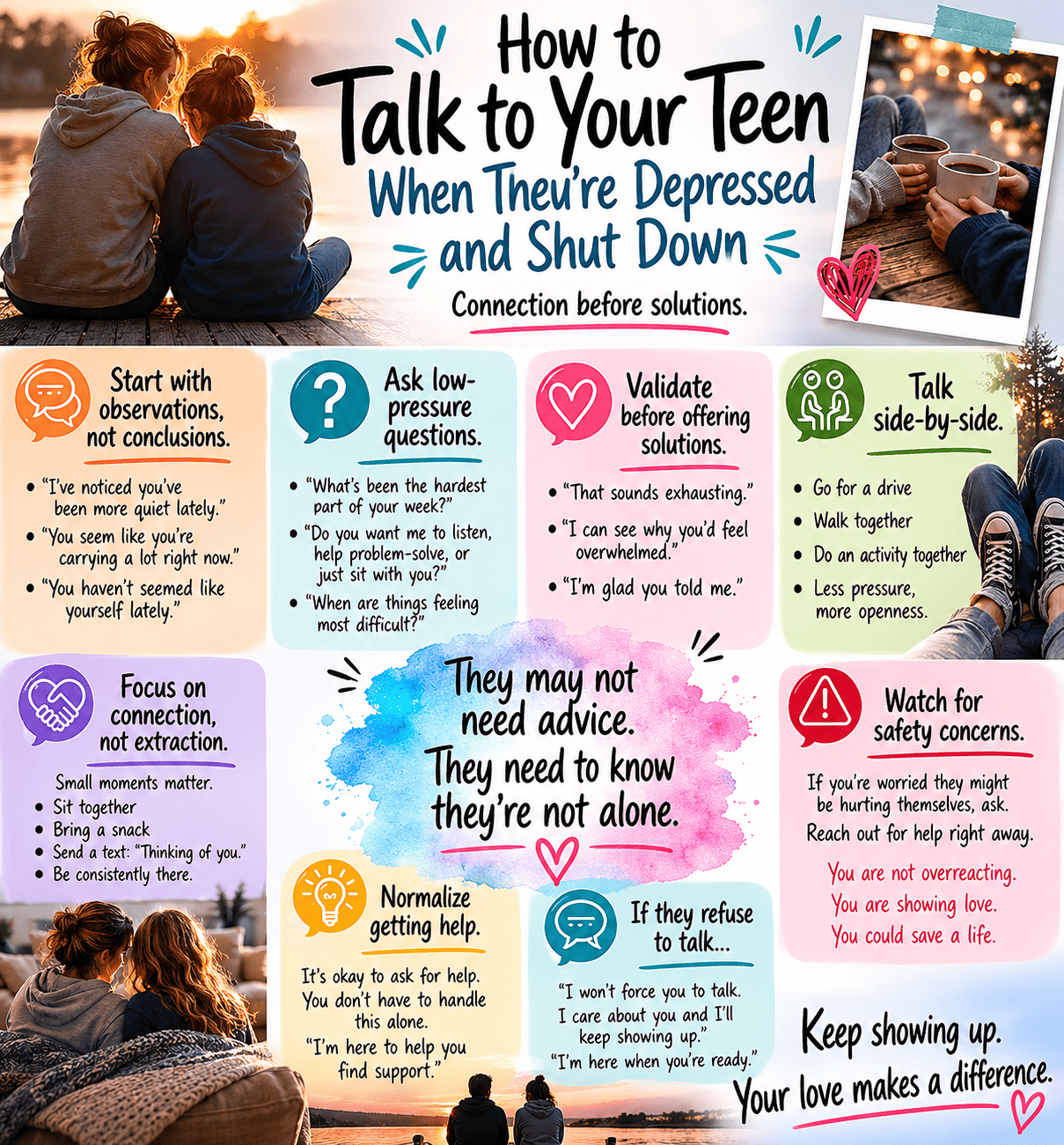
How Families Can Navigate the New Guidelines
As parents, it is important we work with our children’s pediatricians to find the best approach in addressing health/weight/body image in our child. It is clearly stated in the guidelines that parents can tell their pediatrician if they do not want to discuss these topics in front of their child. The parent is the always the advocate until the child learns to advocate for themselves.
Conversations in an annual physical between parents, the child, and practitioner should focus on health-promoting behaviors that are sustainable, realistic, attainable, and accessible. These talks should remain positive, collaborative, focused on health, not weight.
We all know that every family is different and has unique circumstances, including financial, time, and cultural limitations. One thing is for sure that focusing on food variety and balance, eliminating foods as “good” or “bad”, incorporating daily exercise and movement at a young age, and minimizing screen time are good ways to start.
Time and time again we come back to the fact that the best, most effective, safest, and most economical approach to helping our children in having a healthy relationship with food and their bodies is PREVENTION.
It sounds so easy, but it is more time consuming and complicated than one thinks. Ultimately, as parents, we do our very best to raise our children to develop a healthy self esteem, positive body image, and a healthy relationship with food.
There is no magical formula, but we are ultimately the role models and it starts with us. Taking an inventory of our own relationship with food and our body is a great start in order to help our children develop a healthy relationship with their body and have healthy self esteem.
Just remember, as parents, we are doing the very best we can in this moment. Keep educating yourself, working on transforming your own relationship with your body into something positive, despite the number on the scale. And most importantly, emphasize to your children that no matter what their size or weight, they are always accepted and loved by you just the way they are.
As a psychiatric nurse practitioner specialized in the treatment of eating disorders in both adolescents and adults, I have a strong passion for helping parents and families learn to support their children in developing a healthy relationship with their body/weight.
You can reach out for help by going to my website and completing the new patient questionnaire via the link below.